External/internal (as per their relationship to the dentate line)
Grade 1 – protrusion limited to within the anal canal
Grade 2 – protrudes beyond anal canal but spontaneously reduces
Grade 3 – protrudes outside anal canal but reduces fully on manual pressure
Grade 4 – protrudes beyond anal canal and is irreducible
Primary Care Management
Classification
Diagnosis
Diagnosis is by good history taking, visual external inspection and proctoscopy with the aim of confirming the diagnosis and excluding other significant pathology. It is fully appreciated that this can be difficult or not always readily available in the primary care setting.
History:
Examination:
Laboratory:
History:
- Painless, bright red rectal bleeding often following a bowel motion.
- Protrusion of lesions from the rectum.
- Pain may be a feature particularly with thrombosis.
- The presence of altered bowel habit, abdominal pain, weight loss, Iron deficiency anaemia or passage of blood clots or mucous should raise suspicion of other potential diagnoses including colorectal cancer, inflammatory bowel disease, proctitis, fistula or fissure disease (see Scottish Cancer Referral Guidelines.
- Haemorrhoids can also cause incontinence/soiling, anal pruritis and or mass.
Examination:
- Visual inspection looking for external haemorrhoids, skin tags, fissures, fistulas or masses.
- Digital examination and proctoscopy (if skilled to do so) and the patient is not experiencing pain.
Laboratory:
- A FBC would be useful prior to referral if bleeding has been significant or prolonged and may prompt further investigation with endoscopy
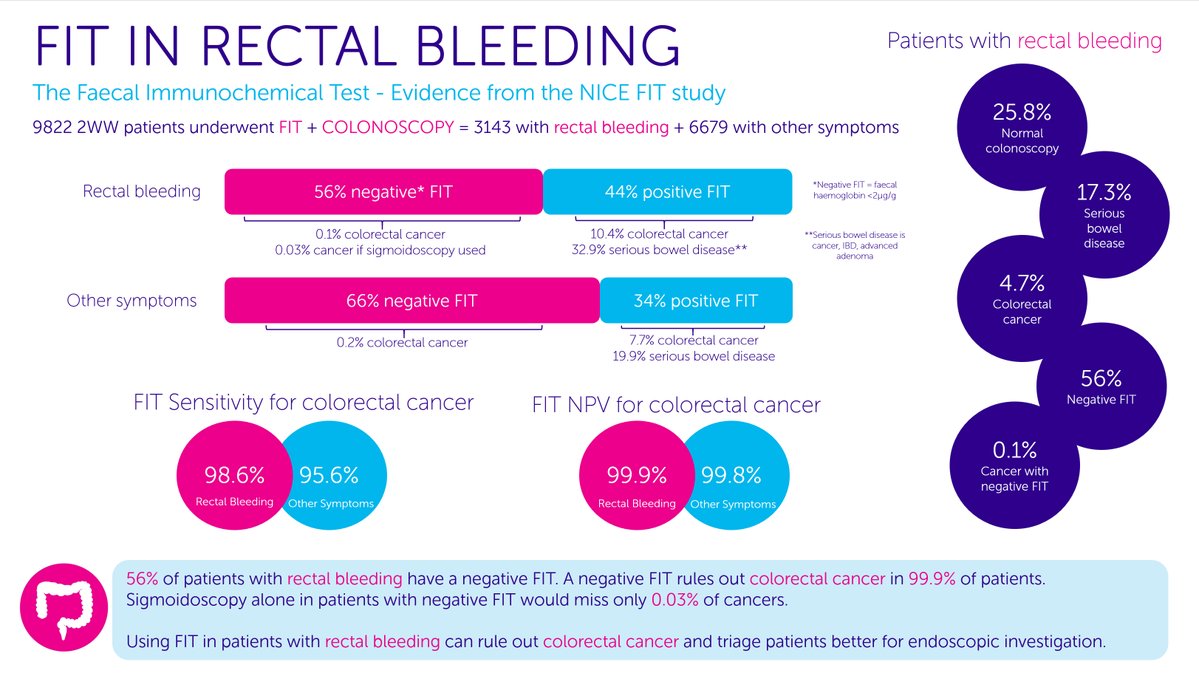
- FIT test should now be requested for all patients with a history of unexplained rectal bleeding, including suspected haemorrhoids prior to referral. It is envisaged that anyone with a positive FIT test, should be referred to the colorectal service initially to get a full colonoscopy as haemorrhoids alone should not raise your FIT. In 'useful resources' are 2 studies which further discuss this, as well as a summary slide from NICE study.
{kind=link}
- With any suspicion of other causes of bleeding, endoscopic assessment should be undertaken. In time, it is hoped that we will set up a sigmoidoscopy and banding service to provide gold standard diagnostic and treatment simultaneously.
- Other symptoms/signs which should trigger either a flexible sigmoidoscopy or colonoscopy include known concomitant conditions (inflammatory bowel disease/ radiation proctitis/ colorectal cancer), presence of red flag symptoms (weight loss, iron deficiency anaemia or altered bowel habit) or other symptoms such as abdominal pain or passage of blood clots/mucous.
Initial management
In the absence of sinister features we recommend initial conservative management for a period of 6 weeks.
Ensure stools are soft and easy to pass
If the person is constipated, consider bulk-forming laxative.
If the person is not constipated:
Give lifestyle advice to aid healing of the haemorrhoid.
Advise on the importance of correct anal hygiene.
Manage any symptoms.
Advise the person that when the haemorrhoid has healed, they should continue with dietary and lifestyle measures to reduce the risk of recurrence.
Ensure stools are soft and easy to pass
If the person is constipated, consider bulk-forming laxative.
If the person is not constipated:
- Advise adequate dietary fibre intake by eating a balanced diet containing whole grains, fruits, and vegetables; this should be done gradually to minimize flatulence and bloating.
- Advise that adequate fluid intake is particularly important with an increased fibre diet to maintain soft, well-lubricated stools and to prevent intestinal obstruction.
Give lifestyle advice to aid healing of the haemorrhoid.
Advise on the importance of correct anal hygiene.
- The anal region should be kept clean and dry to aid healing and reduce irritation and itching.
- Recommend careful perianal cleansing with moistened towelettes or baby wipes, and to pat (rather than rub) the area dry.
Manage any symptoms.
- Offer simple analgesia (such as paracetamol) for pain relief.
- Avoid opioid analgesics (such as codeine) as they can cause constipation, and avoid non-steroidal anti-inflammatory drugs (NSAIDs) if rectal bleeding is present.
- Consider prescribing a topical haemorrhoidal preparations to provide symptomatic relief.
Advise the person that when the haemorrhoid has healed, they should continue with dietary and lifestyle measures to reduce the risk of recurrence.
NHS Inform patient information leaflet. ** Note that not all the surgical options discussed on NHS Inform are available locally - as per information given on summary page.